






By Evans Jona
National Press Foundation Rare Disease Reporting Fellow (2025–2026)
BULAWAYO – When Colette Sophie Morris speaks about her life, she often pauses, as if replaying years of confusion, misdiagnoses and the slow unraveling of a mystery that nearly cost her life. Today, at 43, she lives with systemic lupus erythematosus (SLE), a chronic autoimmune disease that attacks healthy tissues and organs. She remembers her diagnosis clearly: “I was thirty-five when they finally told me what was wrong. That was on the 13th of November 2017.”
For years before that moment, she had been cycling through illnesses that seemed unrelated. “Doctors later told me I had suffered from SLE long before I even knew it,” she said. Her description of the disease is both simple and heartbreaking: “Your immune system turns against your own body. It uses abnormal antibodies to attack healthy cells. It can damage anything – your organs, your skin, your blood. Everything.”
Some of her symptoms are visible; others are not. Excessive sweating, for example, has become a part of her daily life. “If the sweating is too much, it means I am not well,” she explained. “I have to carry extra clothes on a warm day because I become soaking wet.” Fatigue often keeps her in bed for long stretches, and her fingers frequently crack and develop infections, making basic tasks like laundry a battle. Her face, hands and feet sometimes swell without warning. On some mornings, she wakes up partially blind. “But as the day goes on, I start seeing normally again,” she said, as if describing something ordinary.
Her journey to diagnosis spans nearly three decades. She traces the beginning of her ordeal to 1996 when she began collapsing and experiencing fits. “It was a long journey, full of confusion,” she said quietly. “I felt I was sick for too long. At one point I even asked to be started on HIV treatment because I thought maybe everyone was missing something.”
Everything changed in November 2017 when her body suddenly went into severe distress. “My face swelled beneath the eyes and around the cheekbones. My hands and feet swelled. I had maroon marks on my palms and the soles of my feet,” she recalled. Then came symptoms that terrified even the doctors: bloody tears, blood vomit, painful ulcers in the mouth and ears, a butterfly-shaped rash across her nose, and seizures that would not stop. She had been discharged from hospital just two weeks earlier. When she returned, doctors ordered a series of tests. “That is when they said I fit the criteria of SLE,” she said. Her family was called in and informed she had a rare condition. One doctor warned the family to prepare for the worst. “They told us I might live for only six months.”
Before that diagnosis, she endured years of misdiagnoses. She was repeatedly admitted for epilepsy, then treated for diabetes even though she wasn’t diabetic. “One doctor asked me if I had diabetes. I said no, but I had been treated for it,” she said, shaking her head. She later learned she was pre-diabetic. She was also treated for meningitis many times. “They gave me injections even before test results came out,” she said. “Then the results would be negative.” Her confusion, headaches and psychotic episodes were misunderstood. “They said I was going mad. They used the word ‘hysteria,’ and every time I heard it, I cried.”
Reactions at home were mixed. Her immediate family accepted the diagnosis, but relatives outside the home doubted her. “Some thought I was pretending, hiding HIV, or just being lazy because I spent so much time in bed and had lost a lot of weight.”
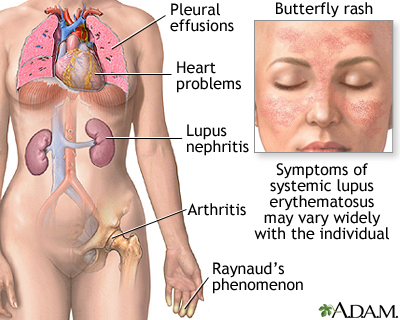
Accessing healthcare after diagnosis brought a new wave of challenges. She had no money for medication or frequent hospital visits. “Even when I had flare-ups, I wouldn’t go because I couldn’t afford it,” she said. Eventually she was referred to United Bulawayo Hospitals, where specialists could monitor her. But information remained scarce. “They didn’t explain much. They showed me the butterfly rash in the mirror, said it meant I had SLE, and then told me to Google what SLE was.”
Medication, for years, was beyond her reach. “My family helped for some time then stopped. Friends helped here and there,” she recalled. Donors through a church network assisted her for three years before the support ended. Tests were expensive and often impossible to afford. Follow-up appointments were equally difficult. Many times she walked long distances to hospitals while hungry or extremely fatigued. “Sometimes I ended up admitted because I was too weak,” she said. Today, she still lives without two major medications used to manage lupus. “I only take hypertension medicine, epilepsy medicine, sleeping tablets and depression medicine.”
Her condition has reshaped every part of her life. She left marriage twice and now lives with her parents and children. She rarely socialises. “I am mostly at home sleeping,” she said. Yet she managed to return to school at 39 and earned a distinction in Biology at the United College of Education despite frequently getting sick. “I lagged behind my classmates. If I had a choice, I would have given up long before halfway. But they refused to let me give up,” she said. Although she finished training, she is still waiting for deployment as a teacher, something she believes is delayed because of her health. “It is stressful seeing my colleagues working while I wait.”
Everyday tasks remain unpredictable. Headaches strike without warning. Tooth infections have led to many removals. She collapses sometimes, suffers chest pain that affects her breathing, and cannot be exposed to much sunlight. Insomnia leaves her exhausted for days. Her memory fails her. She moves slowly. But she has learned a simple rule: “I have learned not to get angry because anger makes inflammation worse.”
Emotional support did not come easily at first. “I used to cry and frustrate everyone around me,” she said. Over time, she built ways to cope. Her mother-in-law became a refuge whenever confusion or illness overwhelmed her. Sometimes she sought treatment without telling her family, just to avoid worrying them. She finds healing in music, prayer, and spending time at the Zimbabwe Red Cross Society. She ministers in children’s church, a role she says brought unexpected strength. “Interacting with children healed me faster than sitting in the main church,” she said. Her family calls her umafa evuke, the one who dies and rises again. “When I recover, you can’t even tell I was ever sick.”
Stigma, however, remains a constant shadow. “People don’t understand what you’re going through,” she said. She rarely discloses her condition unless she believes it will help someone else. She believes communities must learn that rare conditions are not witchcraft and not a curse. “Families should not point fingers looking for someone to blame,” she said. She also warns lupus patients against traditional medicines. “I was told that boosting the immune system can make me worse.”
Morris is now connected to support structures like RADDA and an epilepsy group, which opened her eyes to others living similar lives. But she believes Zimbabwe still lacks emotional, financial and medical support for rare-disease patients. “The voices are there but not loud enough,” she said. If she ever had the chance to address policymakers, she knows exactly what she would ask for: “A national foundation for persons with rare conditions. A place where all the services they need are under one roof.”
She believes rare-disease awareness in Zimbabwe has improved since 2017, especially through social media. She now feels more understood by healthcare workers. “These days they know me. Even at the local clinic, they call me by my name,” she said warmly. The improvements she hopes for are practical: jobs for adults who can still work, free schooling for children, government-funded medication, food vouchers, support groups, and family education. “Love within families facing this ordeal is important,” she said. “When there is love, healing becomes faster.”
Despite everything, she considers herself resilient. “This journey taught me to be tough. The tests I went through were more painful than what an ordinary person could handle,” she said. She knows her triggers now. She pushes herself not to remain bedridden for long. She listens to church audios, writes down scriptures, and drinks water when headaches begin. Her greatest victory remains her education. “Getting a distinction in Biology made me believe that anything is possible, even with a rare condition.”
She thinks about the future of rare-disease care in Zimbabwe often. “I hope that medicine will be available. That everyone will know about these conditions. That a foundation will be opened,” she said, laughing softly as if catching herself dreaming. “Maybe by then I won’t be alive to see it.”
Her message to anyone newly diagnosed is grounded in faith and compassion. “I would pray with them, explain what I know, help them understand their condition,” she said. And then she mentions the scripture she holds closest: “In Isaiah 41:10, God says, ‘Fear not, for I am with you.’ That is what kept me going.”




More Stories
Festive Season Expose Growing Risk For Youth, Missing Girls, Alcohol and Drug Abuse
Faith Leaders Urged to Back Science as Zimbabwe Pushes to End Mother-to-Child HIV Transmission
From Library Discovery to Global Stage, The Young Zimbabwean Challenging Rare-Disease Neglect